Introduction
Orthopedic injuries and musculoskeletal trauma are major contributors to the global burden of disease.1,2 While orthopedic surgery is a vital component of healthcare in developed countries, many low-income countries struggle to provide adequate care for their populations due to limited resources, poor infrastructure, and a shortage of trained professionals.3,4 In low-income countries, musculoskeletal injuries and conditions are often left untreated or are treated inadequately, leading to disability, chronic pain, and reduced quality of life for patients.3,5 These countries also experience a higher burden of orthopedic conditions due to factors such as poor road infrastructure, limited access to safe water and sanitation, and a high prevalence of infectious diseases. In Sub-Saharan African nations, healthcare resources are typically concentrated in dense, urban cities which makes it more challenging to provide surgical care to rural populations.6–8
Addressing the need for orthopedic surgery in low-income countries requires a concerted effort from governments, healthcare professionals, and the global health community. Outreach programs and mission trips are important tools that can mobilize medical experts to provide higher levels of care in rural communities. The Department of Orthopedic Surgery at the University of Zambia is home to FlySpec, a medical charity that facilitates surgical care delivery to the most remote and rural Zambian communities.9 Established in 1982, FlySpec operates with a team of orthopedic surgeons, prosthetists, physiotherapists, and one plastic surgeon. The organization travels via road and air transport to reach rural hospitals where the patient population lacks access to consistent surgical care. Through FlySpec, these patients may benefit from the treatment of burn contractures, congenital deformities, bone infections, and complications of neglected trauma.
The COVID-19 pandemic has had a profound impact on the delivery of healthcare services, including orthopedic surgery, which has resulted in delay of care.10–12 The exact impact of the COVID-19 pandemic on the FlySpec program has not been studied. Conducting a study to examine the current state of the program and how it has operated over the past few years will provide valuable insight into its capacity and future potential.
Methods
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The National Health Research Authority (NHRA) of Zambia approved this study.
We conducted a retrospective study examining FlySpec trip reports from 2018-2022. The sites included in the trip reports span across 7 provinces in Zambia. These were Mukinge Mission Hospital, Chitokoloki Mission Hospital, and Kalene Hills Hospital in the Northwestern Province. The sites in the Northern Province included Chilonga Mission Hospital, Kasama Teaching Hospital, and Mbala General Hospital. The Eastern Province site was St. Francis Mission Hospital and the Western Province site was Lewanika General Hospital. Macha General Hospital, Mazabuka General Hospital, and Livingstone Teaching Hospital comprised the Southern Province sites. Kabwe General Hospital in the Central Province and Mansa General Hospital in Luapula Province were also included. All trip reports were collected by one individual.
The trip reports include valuable information regarding the logistics of clinical care. Pertinent metrics include the number of hospital visits, both by air and by car. Additionally, the operative case volume and quantity of patients seen were scrutinized. These metrics were recorded using the same software across all hospital visits. The reports included other metrics, such as “major operations”, “minor operations”, and “implants used”. However, these were not consistently disclosed in trip reports and showed a degree of provider variability. Therefore, these metrics were left out of the retrospective analysis and omitted from comparison. Mean values and standard deviations were used to analyze differences in the data.
Statistical Analysis
First, the data was classified into two groups. The first group was defined as Pre-COVID-19 and included data from the years 2018-2019. The second group was defined as Post-COVID-19 and included data from the years 2020-2022. Next, the mean value of each metric in both groups was calculated. Following this, the standard deviation for each metric in the Post-COVID-19 group was calculated.
The null hypothesis is that COVID-19 has no effect on FlySpec hospital visits.
Results
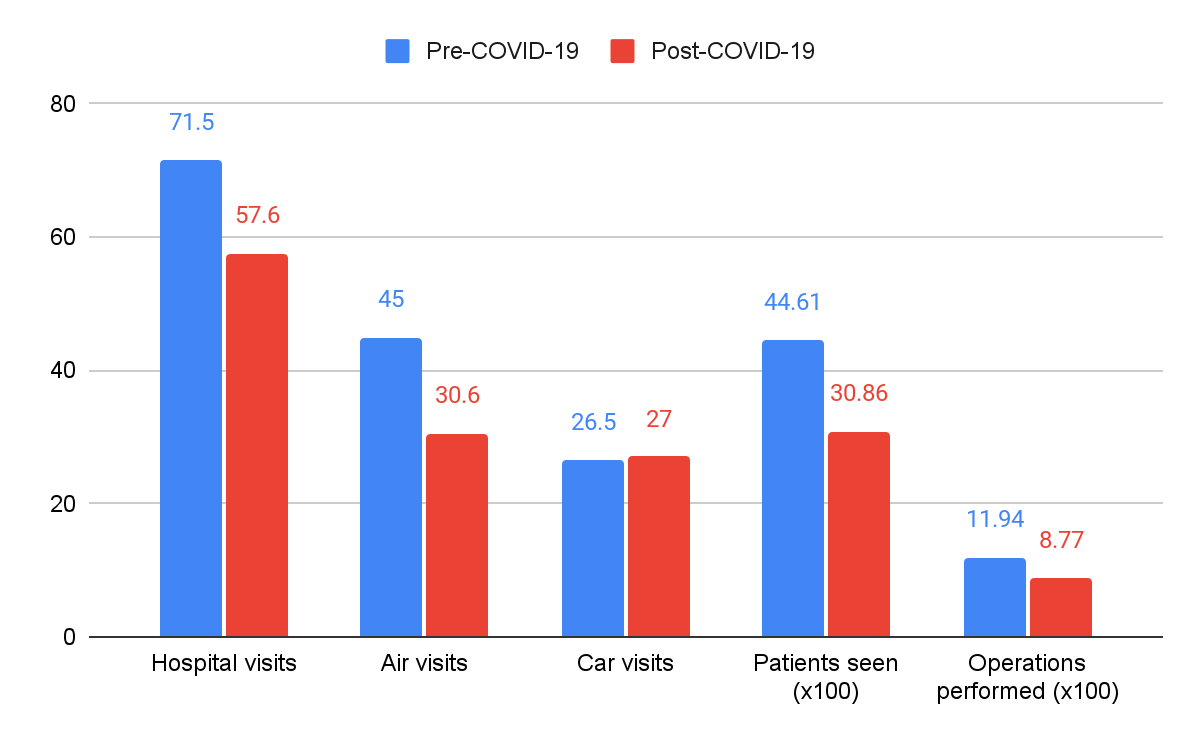
Annual report data can be found in Table 1. The mean number of hospital visits Pre-COVID-19 was 71.5 compared to a Post-COVID-19 mean of 57.6. This decrease is also reflected in the mean number of Pre-COVID-19 air visits, which was 45, compared to a Post-COVID-19 mean of 30.6. On the contrary, the mean number of car visits increased after 2020, with a Post-COVID-19 mean of 27 compared to a Pre-COVID-19 mean of 26.5. These differences highlight the changes in FlySpec practice following COVID-19.
Similarly, the mean number of patients seen and number of operations performed decreased in Post-COVID-19 compared to Pre-COVID-19 (Figure 1). The standard deviation (std dev) for the Post-COVID-19 metrics was also calculated (Table 2). Finally, the mean value difference between Pre-COVID-19 and Post-COVID-19 metrics was calculated to compare average changes. This comparison is shown in Table 3.

Discussion
Our results highlight a difference in the number of hospital visits, patients seen, and operations performed between Pre-COVID-19 and Post-COVID-19 values. On the other hand, a smaller difference was observed in both the number of air visits and car visits throughout COVID-19. This is likely because the determining factor between a car visit or an air visit taking place is the distance of the rural hospital from Lusaka, Zambia. The COVID-19 pandemic had no effect on this distance. Therefore, despite its effects on resource mobilization and healthcare personnel, COVID-19 failed to have a large impact on affecting FlySpec’s mode of transportation to a rural hospital.
The reduction in FlySpec’s clinical activity after 2020 is consistent with published findings that COVID-19 has disrupted clinical services globally.13,14 Elective surgeries and international humanitarian efforts were severely impacted by the pandemic, and FlySpec’s efforts were similarly attenuated.15,16 Patients residing in remote Zambian communities are most likely to be affected by this decrease in FlySpec’s activity. This has likely resulted in further progression of their pathologies resultinging in more urgent clinical presentations. As FlySpec’s clinical activity reaches pre-COVID-19 levels, there may be a corresponding shift in patient morbidity as a result of this delayed presentation. Future studies are needed to accurately assess this discrepancy and to expand on this study’s findings. For instance, analyzing intraoperative data will result in a better assessment of FlySpec’s surgical capacity.
Limitations
This study has several limitations. The FlySpec trip data is reported as annual aggregates as opposed to individual trip details. This is because FlySpec aggregates numerous trip reports and reports them in annual newsletters as opposed to individual trip reports. Efforts to obtain individual trip reports were not successful. This data aggregation has the consequence of heavily reducing the sample size for a given metric. Notwithstanding this, valuable points can be learned from this article regarding the detrimental impact of COVID-19 on FlySpec’s outreach efforts.
Conclusion
FlySpec, a medical charity based in Zambia, has developed partnerships with rural hospitals over the past several decades. The organization has been heavily impacted by the COVID-19 pandemic. There was a decrease in the number of patients seen, hospitals visited, and operations performed Post-COVID-19 compared to Pre-COVID-19. More work needs to be done to further assess the impact of the program in rural communities and to better characterize the challenges faced by the beneficiaries.