INTRODUCTION
The 2015 report by Lancet Commission on Global Surgery highlighted significant disparities in access to safe and affordable surgical, obstetric, and anesthesia (SOA) services globally.1 Notably, it showed that over 90% of the population in low-and-middle-income countries (LMICs) lacked access to safe, timely, and affordable SOA services. To address this burden, countries were advised to prioritize SOA services through the development of National Surgical Obstetric and Anesthesia Plans (NSOAPs) as part of their national health plans.2
In recent years, there has been considerable progress in sub-Saharan Africa, with several countries, including Ethiopia, Zambia, Rwanda, Tanzania, Kenya, and Nigeria developing NSOAPs.2 These efforts aim to fulfil the 2015 World Health Assembly Resolution 68.153 to strengthen emergency and essential surgical care as part of Universal Health Coverage and the sustainable development goals. However, there has been limited evaluation of the implementation status of these plans. We found one evaluation report for the 5-year implementation of the Ethiopia Surgical plan4 but could not locate any mid-term or other evaluation reports for NSOAPs elsewhere.
The United Republic of Tanzania was among the first countries to develop and launch a comprehensive NSOAP in 2018, with support from the GE Foundation, and the Safe Surgery 2020 consortium. The Tanzania NSOAP5 spans a timeframe of 2018-2025 and focuses on several objectives for improving access to SOA services through strengthening the provision of care, training more SOA providers, enhancing referral pathways for emergency and essential surgical care, improving infrastructure and equipment, enhancing data management systems, and advocating for resources to support surgical care.6
This study sought to assess the NSOAP implementation status aiming at understanding the achievements and challenges specifically at the implementation level i.e. the regional level, with the aim of addressing the challenges. Although the survey tool was not constructed to specifically assess each NSOAP objective, it aimed at assessing the Regional Health Authorities understanding of the NSOAP and gather their views on the implementation of the plan and the general status of SOA services in their respective regions.
To advocate for this plan, there is a need to understand the current extent of implementation, enabling and inhibiting factors, steps needed to realize the 2025 target and specific recommendations for future improvement.
METHODOLOGY
Study area
Tanzania has 26 Regional Health Management Teams (RHMTs) composed of the Regional Medical Officer (RMO), Regional Health Secretary, Regional Reproductive Child Health Coordinator, and other departmental managers within the region. The RHMT oversees health activities within their regions including SOA services. The NSOAP was designed to be implemented by RHMTs, hence the expectation that they understand its deliverables.
Design
We carried out a cross-sectional quantitative study using convenience sampling to collect insights through an electronic survey sent to key stakeholders involved in the planning and implementation of SOA services at regional and district levels. Each RHMT was asked to complete one survey tool to describe the status of SOA services in the region from the survey questions. All regions in mainland Tanzania were included in the survey.
Data Collection Methods
We distributed an electronic survey to RHMTs in March 2022 (4 years post-NSOAP launch). The survey tool was organized around the NSOAP objectives: service delivery, referral systems, information management, support services, and the number of available SOA specialists. The survey consisted of closed-ended questions.
The electronic link to the survey was sent to the Regional Medical Officer in each region, and the interviewer followed up with a phone call to ensure that questions were clear to the respondents and the survey was completed timely. We also involved the officials from the President’s Office Regional Authority and Local Government Authority (PORALG) in this assessment since they oversee implementation of health programs at the regional level and were instrumental in ensuring each region responded to this survey.
Data Analysis
We conducted descriptive data analysis and summarized the findings as appropriate using Microsoft Excel. No statistical tests were performed. The findings from the survey were categorized into key NSOAP domains i.e., service delivery, infrastructure and equipment, human resources, information management, finance, and governance.
RESULTS
We sent an electronic survey to all RHMTs in all 26 regions of Mainland Tanzania to gather information on provision of SOA services at the regional/district levels. Each regional team completed one questionnaire. All 26 regions responded to the survey. The Regional Medical Officer is the responsible officer for the RHMT with mandate to guide decisions, but the team is composed of other members including Regional Health Secretary, Regional Reproductive Child Health Coordinator, Regional Dentist, Regional Pharmacist, Regional Laboratory Officer, and other heads of Departments at the regional level. The distribution of the respondents and their roles in the RHMT is summarized in Table 1.
Knowledge of NSOAP policy
When asked about their awareness of the NSOAP, 15 (58%) of the 26 RHMTs were not aware of its existence and only 1 (4%) of the interviewed RHMT acknowledged that they were involved during NSOAP planning in 2018.
Dedicated Ambulance service
16 out of the 26 RHMTs (62%) reported availability of dedicated ambulance services in all or most of their district councils while 10 (35%) indicated that less than half of their district councils had these services.
Surgical Safety Checklist Utilization
When asked about the frequency of WHO Surgical Safety Checklist utilization in SOA facilities, only 2 out of the 26 RHMTs (8%) reported consistent use (i.e. routine use of the checklist for every surgical case in the operating room) in all or more than half of their facilities. 13 participants (50%) noted that less than half of their facilities ever used the checklist and 11 (42%) stated that none of their facilities used the checklist at all.
Surgical Outreach Programs
24 (92%) out of the 26 RHMTs surveyed reported that less than half of their district councils had an established formal surgical outreach program. Only 2 (8%) of the RHMTs reported having an established outreach program in all district councils.
Surgical equipment and supplies
When asked about the proportion of SOA facilities equipped with the necessary equipment, only 9 (35%) of the 26 RHMTs stated that all or more than half of the SOA facilities in their regions possess all the necessary equipment to provide services. 24, (92%) of the respondents reported lack of a fully functional radiology department. All 26 RHMTs (100%) indicated that either less than half or none of the SOA facilities had a functional Intensive Care Unit (ICU). Only 3 (12%) of the RHMTs reported that all or more than half of their facilities have access to biomedical equipment engineering technicians’ (BMET) services.
SOA Service Providers working at the regional level
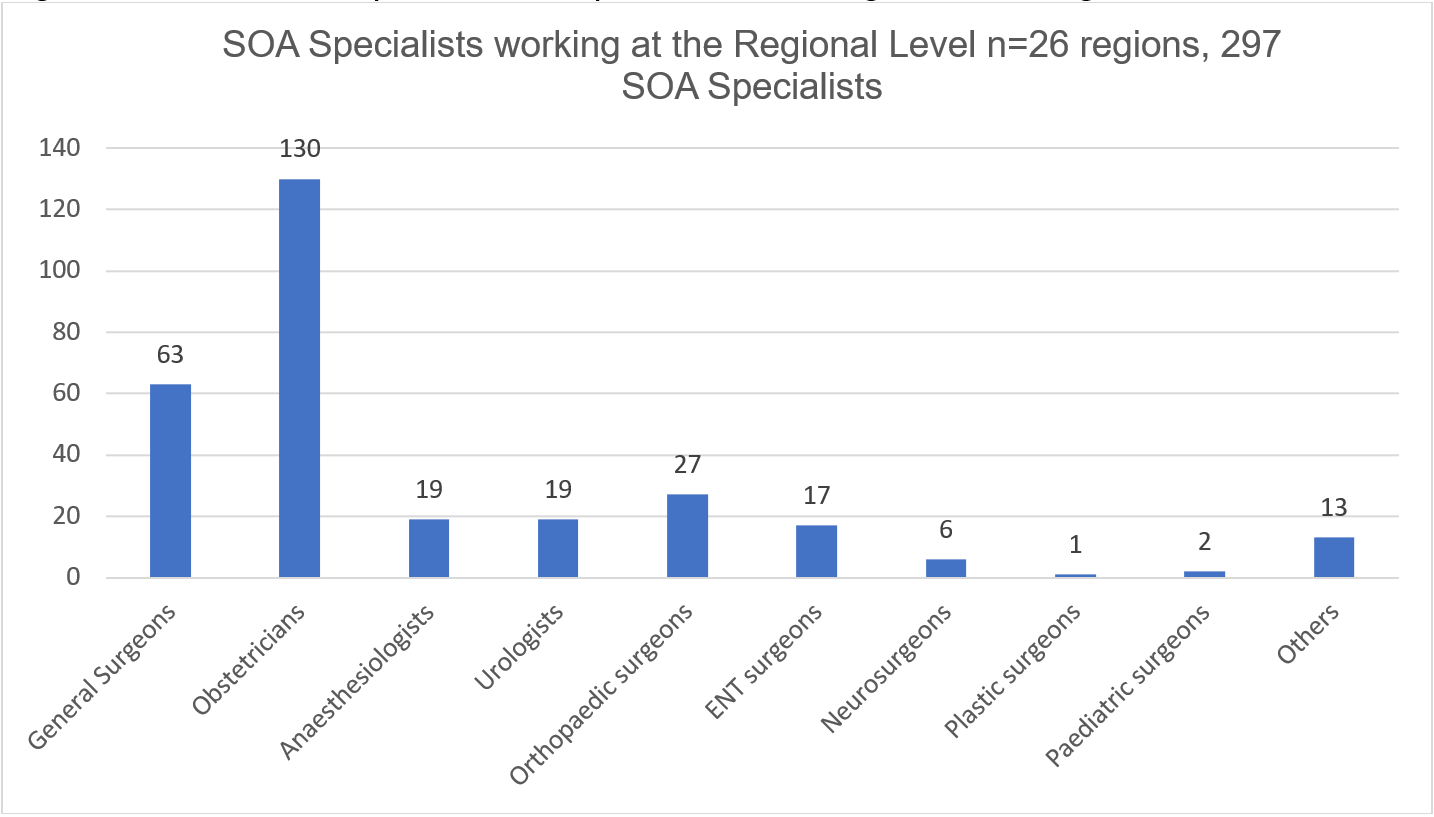
The Tanzanian NSOAP aims to increase the specialist SOA density from 0.46 per 100,000 population in 2017 to 2.27 per 100,000 population by 2025. According to Data from the Medical Council of Tanganyika (MCT),7 there were 1,199 SOA specialists in Tanzania, translating to 1.96 SOA providers per 100,000 population (Table 1). In this survey, we recorded 297 SOA specialists working at the regional level (Figure 1). Majority were Obstetricians (43%) and General Surgeons (21.3%). This number excludes SOA providers at national and tertiary referral hospitals. Seven out of the 26 regions reported presence of anesthesiologists working at the regional level. About a quarter (27%) of the respondents reported availability of SOA training programs in their regions. Since there was no baseline assessment conducted prior to the NSOAP launch, it is difficult to interpret whether these numbers have improved, or not. We correlated this data with the number of SOA specialists recorded in the Medical Council of Tanganyika (MCT) database. The number from the survey captures the SOA specialists working at the regional level specifically in the public sector, while the MCT numbers include specialists at tertiary hospitals and in the private sector. The total number of SOA specialists in the MCT database is referenced in Table 2.

Governance
Only 7 out of the 26 RHMTs interviewed (27%) reported inclusion of SOA activities in their Comprehensive Council Health Plans (CCHPs). Only 3 of the 26 RHMTs (12%) were involved in NSOAP dissemination meetings and also 3 of the RHMTs interviewed (12%) had appointed a dedicated NSOAP coordinator at the regional level.
DISCUSSION
The Tanzania MOH launched the NSOAP in 2018 aiming to systematically strengthen SOA care in Tanzania over seven years. This study represents the first national assessment of this policy document.
Regarding SOA service delivery, the survey highlighted gaps in service provision at the district level. Referral systems were found to need strengthening and this was similar to findings in other LMICs emphasizing the need to strengthen this area.8
Reducing maternal mortality is a key priority of the Tanzanian NSOAP. Availability of CEmONC services was limited, with a low percentage of health centers offering a full range of services, including c-section and blood transfusion services. Previous studies in Tanzania and elsewhere showed similar gaps, demonstrating a need for more focused efforts to improve SOA services.9 Although there was an overall increase in the number of health facilities, shortages in critical services such as anesthesia and critical care persisted as previously.9
According to MCT data7 there was an increase in the number of SOA specialists (Table 2) (1.96 per 100,000 population) compared to 0.46 per 100,000 population when the NSOAP was launched,6 possibly due to new graduates from the ongoing scale-up of post-graduate programs in various medical schools, but the density remained low compared to the Lancet Commission standards (20 SOA Providers per 100,000 population.1 However, these results may not necessarily reflect the targets set during the NSOAP launch.5 Fewer of these specialists were working at the regional level (Figure 1).
The low awareness level of the NSOAP among the respondents is concerning, highlighting the need for enhanced efforts in NSOAP dissemination to key stakeholders. Without adequate awareness, it is challenging to align the NSOAP objectives with the regional plans. The limited participation of RHMT members in the NSOAP development process raises questions about the inclusivity of stakeholders in shaping the plan. Active involvement and collaboration among key decision-makers at the regional level are essential for the effective implementation and sustainability of services. The lack of a governance structure at the regional level, as exampled by the absence of NSOAP coordinators is a significant barrier to the implementation of this plan.
The availability of dedicated ambulance services in most district councils is encouraging, but there is a need to ensure consistent access and optimal utilization of these services. This includes addressing challenges such as infrastructure, resources, and coordination between ambulance services and healthcare facilities, as reported in a similar setting in Malawi.8
The WHO surgical safety checklist is recommended by the WHO to improve surgical quality and outcomes. The low utilization of the WHO Surgical Safety Checklist highlights a critical patient safety concern. Efforts should be directed toward promoting the widespread implementation and consistent use of the checklist across SOA facilities. To improve access and equity in surgical care, it is essential to strengthen surgical outreach programs, address infrastructure gaps, and ensure the availability of appropriate equipment and supplies in all facilities providing SOA services. These best practices have been implemented in some settings in Tanzania as evidenced by the Safe Surgery Project10–12 calling for country-wide scale-up of such interventions. The findings regarding the functional radiology departments, laboratories, and intensive care units in SOA facilities indicate areas of concern with a need of ensuring availability of these critical components in promoting quality and safety of surgical procedures, as highlighted in one study in a similar low-resource setting.13
The low-density ratio of SOA providers and the limited presence of anesthesiologists at the regional level highlights the need for strengthening the workforce capacity. Increasing the number of SOA specialists and ensuring their distribution across regions is essential in improving the delivery of safe services. The low percentage of SOA training programs indicates the need for greater emphasis on training and integration of SOA services at the regional level, as recommended in the NSOAP.
The limited involvement of regions in NSOAP dissemination and lack of dedicated NSOAP coordinators within the Ministry of Health raised concerns about the coordination and implementation of the plan at the regional level. Effective communication, coordination, and leadership are crucial for the successful execution of the NSOAP. It is important to follow the NSOAP development framework and pay attention to the key barriers in the translation of policy to practice.14,15
Study Limitations
Due to limited time and resources, we could not use more interactive approaches such as focused group discussions, direct observations, or field visits. In addition, published literature might be subject to bias, may not cover the latest developments, and might not capture the full range of perspectives. As with many large-scale policy projects, it is challenging to attribute improvements in SOA services exclusively to NSOAP implementation since the NSOAP monitoring and evaluation framework had not been established. Furthermore, patient and community perspectives on the status of SOA services were not included and we did not also assess the impact of the COVID-19 pandemic in delaying the plan implementation.
CONCLUSION
Findings from this analysis revealed important insights into the current state of SOA services and the implementation of the NSOAP in Tanzania.
The findings highlight areas of strength and areas that require targeted interventions for improvement. To achieve the goals outlined in the NSOAP and enhance the overall quality and accessibility of SOA services, concerted efforts are needed at both the national and regional levels. Collaboration, capacity-building, infrastructure development, and continuous monitoring and evaluation are vital for the successful implementation of the NSOAP and the improvement of SOA services at the regional and district levels.
Several areas requiring attention and improvement were identified, including gaps in capacity for service provision, workforce shortage, infrastructure and equipment, coordination and governance, and capacity building. Despite some positive aspects, such as an increase in the number of general healthcare facilities and a modest increase in the density of SOA providers, there are several challenges highlighted that need to be addressed to enhance the delivery of safe and effective SOA services in the country and to achieve NSOAP objectives.
In general, there is a paucity of literature specific to NSOAP implementation in Tanzania, highlighting the need for more research and evaluation studies to generate additional information.
RECOMMENDATIONS
Based on the discussion and findings, the following specific recommendations are proposed in ensuring that the NSOAP will be implemented effectively as intended:
NSOAP Dissemination: There is a need to ensure that the NSOAP is disseminated to all key stakeholders especially those working at the implementation level i.e., the regional and district levels.
Monitoring and Evaluation of the NSOAP Implementation: There is an urgent need to fast-track the implementation of the NSOAP monitoring and evaluation implementation framework. This will allow better collection of SOA related indicators to be able to track performance of the services in general such as types of surgeries, anesthesia details, patient outcomes and other gaps in SOA service provision. These indicators will be useful in tracking progress of achievement of the NSOAP objectives.
Strengthen capacity at the district level: Efforts should be made to strengthen the capacity of SOA service provision at the district level. This includes improving referral systems, expanding the availability of CEmONC services, addressing shortages in critical areas like anesthesia and critical care, and ensuring a robust supply chain for SOA-specific supplies and consumables.
Increase the number of skilled SOA professionals: To meet the growing demand for SOA services, there is a need to increase the number of skilled healthcare professionals, particularly anesthesiologists. Strategies should be implemented to improve the recruitment, training, and distribution of healthcare professionals in the SOA field. Specific actions should be taken for critical areas such as anesthesia and critical care through sensitizing medical students to aspire for these specializations and provision of motivation packages and sponsorship opportunities for those who wish to specialize in these cadres.
Enhance coordination and governance: The coordination and implementation of the NSOAP should be strengthened at both the national and regional levels. This includes increasing awareness of the plan among key stakeholders, fostering greater participation and engagement in the planning process, improving communication and coordination among healthcare professionals and decision-makers, and appointing dedicated NSOAP coordinators at the regional level.
Promote standardized training and guidelines: Efforts should be made to develop standardized training programs for health providers in the SOA field, including establishment of surgical outreach and mentorship programs to lower-level facilities. SOPs and clinical guidelines for SOA should be developed and coordinated at the national level to ensure consistent quality of care. Training programs, mentorship and continuous monitoring should be encouraged to promote adherence to safety protocols, such as the WHO Surgical Safety Checklist.
Secure funding and evaluate progress: More aggressive efforts are needed to secure funding for the implementation of the NSOAP. Regular evaluations should be conducted to assess the progress made, identify existing barriers, and revise the plan to reflect the current reality on the ground. There is a need to continue to advocate for NSOAP funding and identify donors who will be able to provide funding for the activities outlined in the NSOAP. Otherwise, most activities in the plan will never be implemented to the same extent as stipulated in the plan.
Revitalize the NSOAP Technical Working Group: The NSOAP Technical Working Group at the national level plays a vital role in coordinating partners involved in SOA projects. Efforts should be made to revitalize the group and ensure its active participation in driving the implementation of the NSOAP.
NSOAP Mid-term Evaluation: we recommend a more robust evaluation of NSOAP implementation through a mid-term evaluation exercise using more interactive methods to assess ALL NSOAP strategic objectives and activities outlined in the plan, and hence show a more realistic picture of the state of implementation to date.
Key Lessons learnt
Baseline Assessment: A critical aspect often overlooked in policy implementation is the necessity of conducting a comprehensive baseline assessment. This foundational step serves as a crucial benchmark, providing insights into the existing state and capacity within the healthcare system. In our case, a baseline assessment would have helped to establish the status quo and provide a more meaningful understanding of the availability of services, infrastructure, and human resources at the outset to be able to track progress over time. It is therefore critical to invest time and resources in thoroughly understanding the existing healthcare landscape before embarking on an ambitious policy endeavour, such as the NSOAP.
Policy Dissemination: It is essential to ensure that the policy is widely disseminated to all key stakeholders, especially those that are involved in the day-to-day implementation of activities related to the plan such as the RHMTs. In our case, the limited participation of RHMT members in the NSOAP development process and their general lack of awareness about the plan, might have contributed to the slow implementation of the plan at the ground level.
Funding: The successful implementation and sustained impact of the NSOAP is heavily dependent on a robust and sustainable financing plan. Adequate funding is the lifeblood that ensures the realization of proposed interventions, the improvement of healthcare infrastructure, and the enhancement of SOA services. Creating a sustainable financing plan involves multi-stakeholder collaboration. The financing plan should be intricately linked to the policy objectives outlined in the NSOAP. Advocacy efforts at both national and international levels are integral to securing sustained funding for the NSOAP.
Governance Structure: Without effective leadership at the implementation level of the plan, success is unlikely to be achieved. The absence of NSOAP coordinators at the regional level is a significant barrier to plan implementation. Establishing a governance structure at the regional level and appointing dedicated coordinators will enhance the effectiveness of the NSOAP.
Monitoring and Evaluation Framework: Establishing a monitoring and evaluation framework for the NSOAP is essential. This would enable tracking progress, attributing improvements in SOA services to NSOAP implementation, and identifying areas that require adjustments.