Introduction
A gastrointestinal bezoar is a mass that develops through the accumulation and subsequent hardening of indigestible materials within the digestive tract. Based on their component, they are classified into four main types: phytobezoar (fruit and vegetable fibres), trichobezoar (hair), lactobezoar (undigested milk concretions) and pharmacobezoar (medications).1 On the other hand, a Lithobezoar is defined as an accumulation of ingested stones within the gastrointestinal tract. These small pebbles or stones conglomerate in the gastrointestinal tract to cause mechanical bowel obstruction. This is usually associated with Pica; an eating disorder characterized by ingestion of non nutritive substances.2 Lithobezoar is a rare cause of mechanical intestinal obstruction in children and only a few cases have been reported from other countries.3–14 Up until 2022, only thirteen cases were reported in paediatric patients worldwide.13 In Africa, similar paediatric cases were reported in a 5-year old Nigerian boy,15 a 15-year-old Rwandese boy16 and 4 year old Sudanese boy.17 In Zambia, lithobezoar still remains an unknown cause of intestinal obstruction as there is none on record. In this patient, it affected the whole colorectal segment unlike most of the cases reported in literature. It is for this reason that we present a case report of a 7-year-old girl who presented with features of acute intestinal obstruction following massive ingestion of small stones for an unknown period of time.
Case presentation
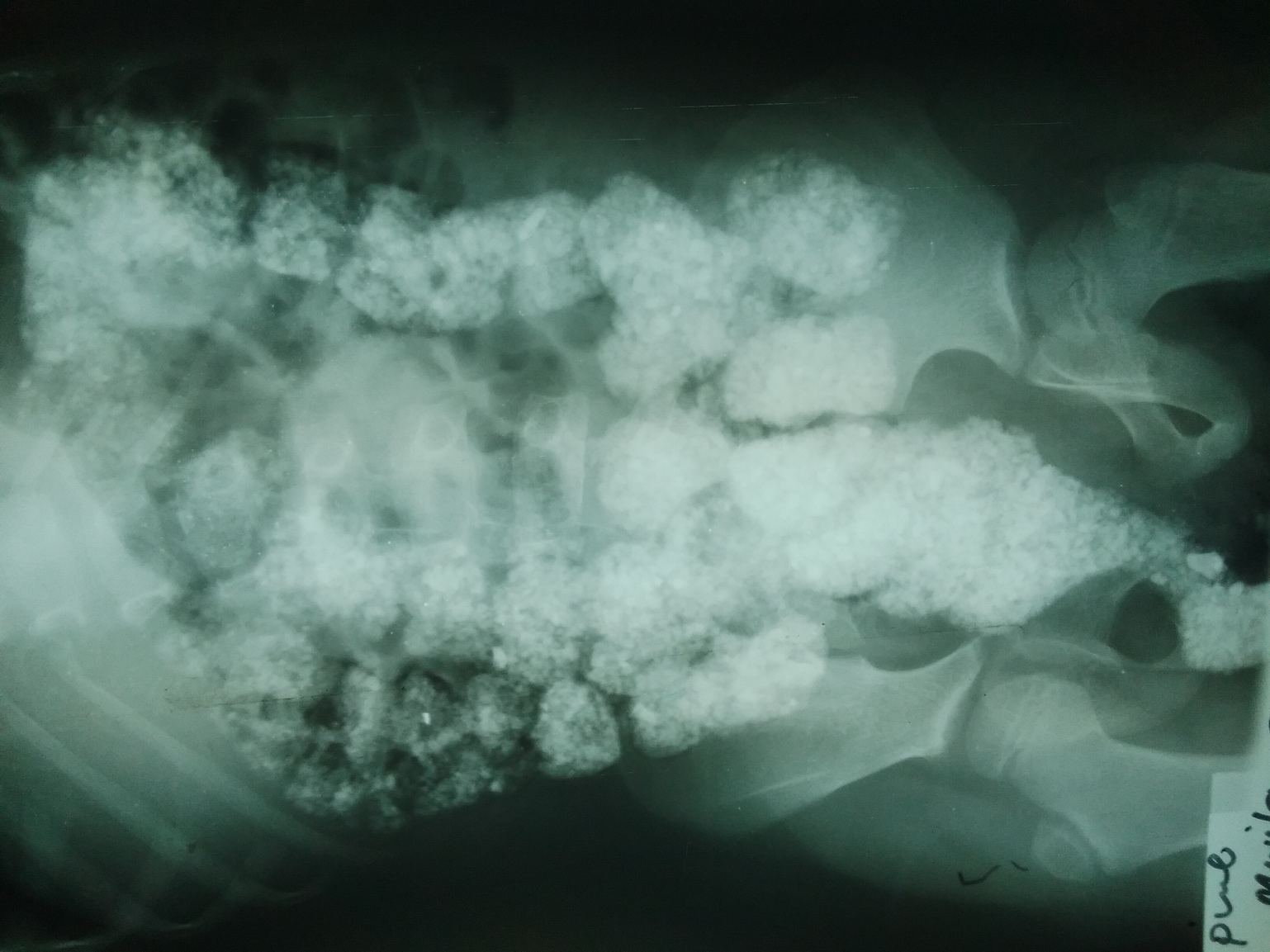
A 7-year-old girl was brought into the outpatients department by her parents with a history of ingestion of small pebbles for an unknown duration. She was complaining of constipation, abdominal distension and pain for 2 days. She was also reported to have had painful defecation and had passed out some small stones mixed with stool 2 days before. There was no history of vomiting or fever. There was no history to suggest any form of psychiatric illness. She admitted to having had taken some small stones orally together with some friends for an unknown period. She was said to be in her second grade with an average performance. She had six other siblings and was living with her biological parents from a low social economic class. There was no history of previous hospital admissions. Her birth and psychomotor development were reported to have been normal. On examination, she was not in any distress. The nutrition status was good and clinically, she was not pale. There was moderate lower abdominal distension though it was soft with some tenderness in the lower region. Multiple irregular masses were palpated in all the quadrants and also had increased bowel sounds. On inspection, small matted stones were protruding from the anus. Digital rectal examination revealed multiple compacted prickly small stones in the rectum. All the other systems were normal. Full blood count was essentially normal with a haemoglobin level of 11.3g/dL. Iron and B12 blood levels were not done due to inavailability of equipment to use. Plain abdominal X-rays showed multiple compacted radiopaque masses of various sizes involving the whole colon from the caecum all the way up to the anus with a funnel shaped mass filling the entire rectum. A diagnosis of mechanical intestinal obstruction secondary to lithobezoar was made. Manual evacuation of the highly compacted rectal stones was done under sedation until semi solid stool mixed with stones started coming out. This was followed by a water enema. She continued to pass voluminous stool mixed with stones for three days. The abdomen became soft with no signs of peritonism. A repeat X-ray on the 5th day showed a normal abdomen and so the patient was discharged. Emphasis was made to the parents to ensure that no further stones were ingested.

Discussion
It is quite evident that this patient had been ingesting small stones for a long time to accumulate such a large quantity before she became symptomatic. The most common risk factors associated with bezoar are pica, behavioural disturbance in young girls, psychiatric illness, intellectual disability and low socioeconomic status.8 She was the sixth child of her family from a low socioeconomic status that could explain her compulsive behaviour of pica. Paediatric lithobezoars are more common in boys than in girls.4 Despite geophagy, the deliberate consumption of soil, being a common practice amongst the world’s poorer or more tribally oriented people of the tropics,18 paediatric lithobezoar still remains uncommon in Zambia. As shown above, up until 2022 only thirteen cases of paediatric lithobezoar were reported in literature worldwide. There is an association between Pica and iron deficiency anaemia,18 though it was not the case in this particular one as the haemoglobin was at 11.3g/dL. Palpation of a prickly mass on rectal examination is known as the colonic crunch sign. The presence of multiple radio opaque masses in the abdomen is referred to as corn on cob sign and is pathognomonic to lithobezoars. These two are key to the diagnosis of colonic lithobezoars10 and were also demonstrated in this patient. A conservative approach to the management of this patient was in agreement with all the other paediatric cases of lithobezoars reported. There is need to review our local hospital records as some cases of colonic bezoars may have gone unreported considering the high prevalence of geophagia in Africa.
Conclusion
From the above presented case, it can be concluded that Pica can complicate into acute intestinal obstruction requiring hospital intervention. Conservative management is the best approach in paediatric patients. This involves manual evacuation and enema administration coupled with oral laxatives. Paediatric surgeons should consider Lithobezoars as one of the causes of intestinal obstruction in children. The colonic crunch and corn on cob signs are key in making the diagnosis.