
Introduction
Breast Cancer (BRCa) is the most common type of cancer among women worldwide.1 Managing BRCa in our continent has been challenging for various reasons. Many patients with breast cancer living in low and middle-income countries present at an advanced stage of the disease.2 This, coupled with the fact that treatment options are often limited and not easily accessible, makes BRCa treatment difficult in resource-limited areas.
Surgery is the most common mode of treatment for BRCa in Africa.3,4 According to a continent-wide review of surgical management of breast cancer,4 Breast-Conserving (BC) surgeries and lumpectomies are rarely performed in our continent due to the advanced presentation of the disease and limited availability of radiotherapy.
Lymph node metastases are the strongest predictor of recurrence and survival in women with BRCa. The histologic status of the SLN represents the status of the entire axilla. Thus, a negative SLN predicts the negativity of the remaining axillary nodes and eliminates the need for extensive axillary dissection.5 With a low false negative rate of 5-10% and a high sensitivity rate of 90-95% in the detection of cancer in the lymph node basin, Sentinel Lymph Node Biopsy (SLNB) has become a standard of care.6,7 Eligible patients include those with early T1-T2 invasive BRCa and clinically negative axillary nodes.8
When used appropriately, SLNB can save 70% of women with clinically negative axillae from undergoing a complete axillary dissection and the associated complications.5 The advantages and safety of SLNB were further demonstrated by the NSABP B-32 trial, which concluded that the survival advantage of SLN surgery alone is equivalent to SLN and additional ALND in cases where the node is negative.9 Even in patients with SLN micrometastasis (< 2 mm) and T1-T2 invasive BRCa, studies such as the International Breast Cancer Study Group trial 23-01 (IBCSG 23-01) have shown that there was no statistically significant difference in OS rate between those treated with SLNB only and those that underwent ALND10
Regardless of all the above-stated advantages of SLNB, it is not a widespread practice in our continent. Our institution (MCM Comprehensive Specialized Hospital) is one of the centers in Ethiopia where SLNB is performed. The practice was initiated in 2020 with the training and supervision of an oncologic surgeon from abroad. This study aims to assess the validity and benefit of SLNB in the absence of radionuclide dye using only blue dye in identifying lymph node metastasis and to share our institutional experience with other surgical centers. With the availability of neo-adjuvant chemotherapy and radiation therapy in Ethiopia shortly, we believe that it is of paramount importance to get accustomed to such standard practices. To this end, we hope our experience with SLNB is encouraging and may be reproducible in other surgical centers in our country and our continent.
Methods
Study design and setting
Retrospective, cross-sectional study at MCM Comprehensive Specialized Hospital, Addis Ababa, Ethiopia, from October 1, 2020 to October 30, 2023.
Study participants
Patients diagnosed with invasive BRCa that had a complete clinical evaluation, routine laboratory exams, and CA15-3, imaging with mammogram and/or breast ultrasound, Chest X-ray/chest CT, abdominal ultrasound or CT with contrast, and histopathologic exam results from core needle biopsy were included in the study. Patients with gross axillary disease, inflammatory BRCa, and those having incomplete data were excluded.
Sample size
Twenty individuals diagnosed with BRCa at various stages underwent SLN mapping between October 2020 and October 2023. Two patients were removed from the study due to insufficient data.
Procedural detail
All procedures were performed by a consultant surgeon and senior surgical residents under the direct supervision of an oncologic surgeon with more than 30 years of experience, with the primary intention of transferring the skills of SLNM. Before each procedure, written informed consent was obtained. The primary surgical treatment was either MRM or breast-conserving therapy (BCT), which was based on the patient’s ability to afford to go abroad for radiation therapy.
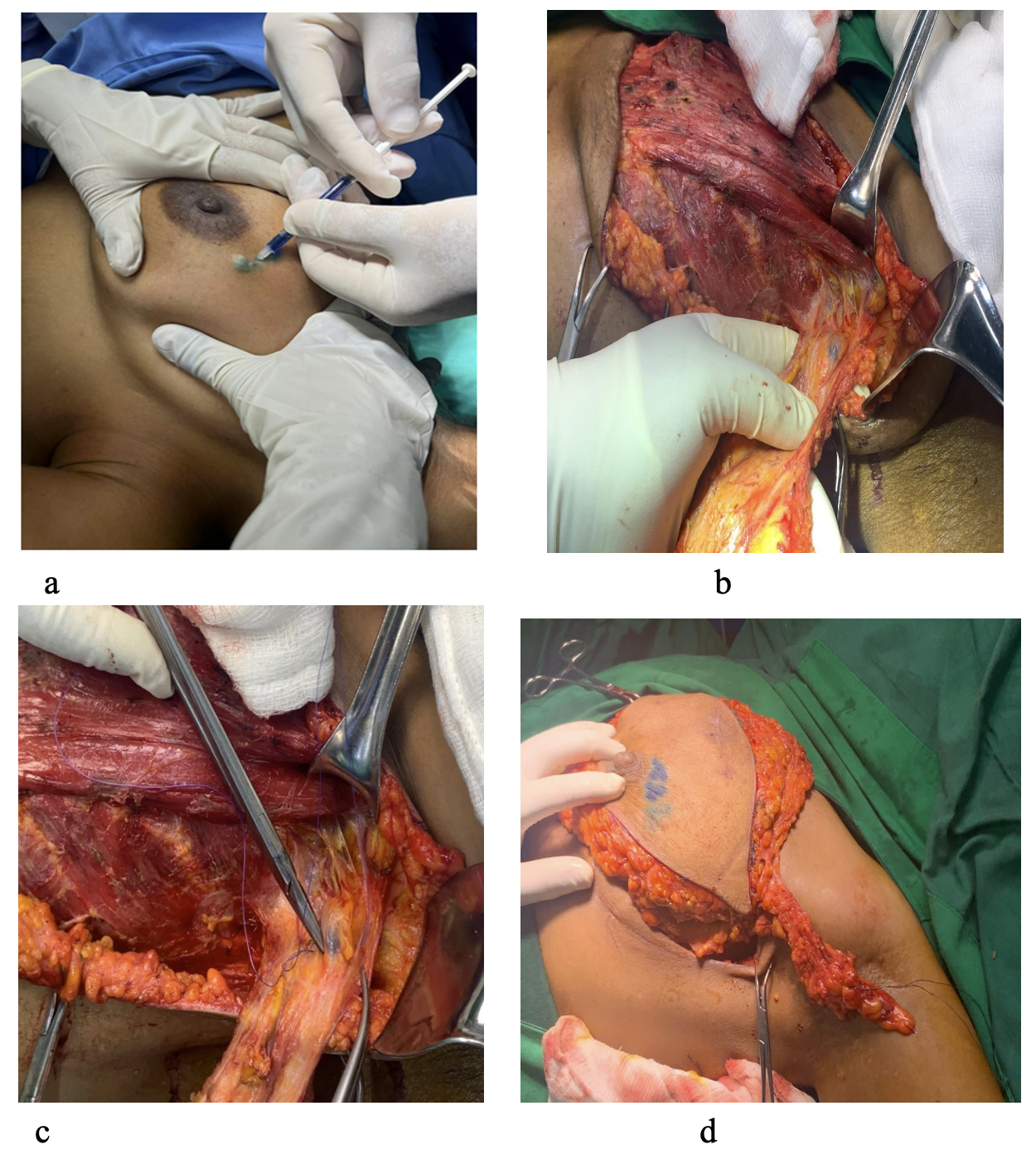
SLNM was performed in the operating room under general anesthesia. Two milliliters of methylene blue dye were used for intradermal, sub-areolar injections using a tuberculin syringe, and 3ml peri-tumoral injections using a 27 G needle (Figure 1a). Maintaining low pressure and slow injection to avoid rupturing the lymphatic channels were the critical steps of the procedure. The whole procedure took about 7 minutes. The injection site was manually compressed and gently massaged towards the axilla for 5 minutes before the skin incision. Dissection through the subcutaneous tissue and clavipectoral fascia into the axilla was performed through the most lateral incision of planned mastectomy or a separate incision just below the axillary hairline for BCS. All blue-stained lymph nodes were harvested and marked with stitches in the specimen as 1st, 2nd, and 3rd SLNs before placing it into formalin because formalin may remove the blue stain from the SLNs (Figure 1 b,c,d). Following SLNM and SLNB, routine level I and level II ALND was carried out for all patients. Level III ALND was performed only if gross disease in the axilla was identified during surgery. Lateral and medial drains were placed before the completion of the procedure.

Postoperatively, patients were discharged after 1 to 2 days in hospital stay and advised for follow-up in the clinic within 3 -7 days after surgery. During follow-up, wound and seroma assessment was performed, and drains were removed when the output was less than 30 ml. Cases were discussed postoperatively during tumor board meetings if subsequent adjuvant therapy is clinically indicated. Subsequent postoperative follow-up was performed at three months, six months, and one year. Every year, women underwent mammography and/or chest wall/axillary ultrasonography (if clinically appropriate). Findings of clinical recurrence were subjected to imaging and Core Needle Biopsy (CNB).
Pathologic examination
All SLNs were ultra-staged with serial multi-level sectioning, embedded in paraffin, and stained with Hematoxylin and Eosin (H&E) per laboratory protocol. Macro-metastasis, micro-metastasis, and isolated tumor cells (ITC) were defined as more than 2 mm, more than 0.2 mm but less than 2 mm, and 0.2 mm or less in size, respectively (Figure 2 a, b, c). Breast tumor specimens were routinely sent for hormone receptor testing to ascertain the status of the estrogen, progesterone, and HER2 receptors. Non-SLN metastases, in the absence of SLN metastases, representing skip metastases, were also evaluated. Cytokeratin immunohistochemical (IHC) staining was not routinely performed.

Data collection
Patient’s medical records were reviewed, and clinical, pathological, and outcome-related characteristics were investigated. The variables studied were age, treatment of primary tumor, number of SLNs identified, number of SLNs positive for tumor, the total number of LNs identified from ALND, final pathology of the specimen, tumor size, tumor grade, hormonal status, and HER2 receptors.
Data analysis
Data was collected and coded using Microsoft Excel. Descriptive statistics were used, and values were expressed as mean and frequency (percentage).
Ethical considerations
Ethical clearance was obtained from the internal review board of Myungsung Medical College.
Results
Twenty11 female BRCa patients with clinically unremarkable axillae had undergone SLNM from October 1, 2020, to October 30, 2023. The median age was 47.75 years ± 13.33. Preoperatively, 10 (50%) of the patients had right BRCa, 9(45%) patients had left BRCa, and 1(5%) had bilateral BRCa. To treat the original tumor, the majority of patients (85%, 17) underwent MRM, whereas (15%, 3) underwent BCS (Table 1).
The final histology result of the breast tumor in all cases was invasive ductal carcinoma. Fifteen patients (75%) tested positive for ER, 60 %12 of patients tested positive for PR, and 30 %6 for HER 2 positive. The majority of patients, 50%10 had T2 tumors (> 2 cm but ≤ 5 cm), and 50%10 had T1 tumors (≤2 cm). Eleven patients (55%) had a Grade 1 tumor, 40 %8 had a grade 2 tumor, and 5%1 had a Grade 3 tumor. No distant metastases existed in any of the patients. The majority of patients (70 %, 14) experienced no complications following surgery; however, two patients reported numbness near the surgical site, and four patients developed a seroma.
Neoadjuvant chemotherapy was administered to 40%8 of the patients, whereas adjuvant chemotherapy and radiation therapy were administered to 60%12 and 65%13 of patients, respectively. Fifteenth patients (75%) are currently receiving hormone therapy.
During the pathologic evaluation of the axillary lymph node dissection, one patient had nine lymph nodes, 16 patients had between 10 and 15 lymph nodes, and three patients had more than 15 lymph nodes. The average total ALNs is 13.6. Six (30%) of the patients had positive SLN status; three had metastasis only in the SLN, while the remaining three also had non-SLN metastasis in addition to the positive SLN.
All of the patients’ sentinel lymph nodes were successfully found during surgery. In our study, the blue dye procedure had a 100% success rate for identifying SLNs. Seven patients (35%) had 1 SLN, Four patients (20%) had 2, Six patients (30%) had 3, one patient (5%) had four, one patient (5%) had 5, and another patient had six (5%) SLNs extracted Table 2).
Discussion
SLNB is the currently accepted standard of care for axillary staging in BRCa with clinically negative axilla. However, performing SLNB alone is not feasible in resource-limited setups like sub-Saharan Africa, where a frozen section is not widely available. On top of that, the utter lack of radiation therapy centers makes post-operative axillary radiation almost impossible for this category of patients. Hence, the current practice is to perform complete ALND for all patients presenting with invasive BRCa. This has resulted in a scarcity of data on SLNM in managing BRCa in this part of the continent.
There is a growing policy change in this part of the continent focused on enhancing the treatment of non-communicable diseases such as BRCa. In line with this, strides are being made towards making advanced treatment options such as radiation therapy available in different parts of this continent. As a result of the economic growth and advancements in technology and education seen in our country, currently, many patients diagnosed with invasive BRCa tend to have a better grip on their situation. They are well aware of the various treatment options available. Most patients even opt for more conservative approaches; some pursue further adjuvant treatment abroad. It is only a matter of time before these diagnostic and therapeutic options are available in this continent. This makes the practice and development of standard surgical skills of SLNM a necessity for surgeons in these regions. Based on our experience in our facility, we believe SLNM is a safe, inexpensive, easily reproducible skill that requires a relatively short learning time with the right trainer.
The practice of SLNM was started in our facility in 2020. It was initially introduced by a senior oncologic surgeon from the US with the intent of transferring this skill to residents and consultant surgeons to eliminate the traditional routine practice of ALND for every patient with invasive BRCa and avoid the various morbidities associated with it.
The primary option of treatment was MRM, but BCT was also offered for patients who could afford to go abroad for radiation therapy. The rate of BCT in our study was 15%. Even though this value is much lower than the rate seen in developed countries, which ranges from 58 to 66.8 %,12,14 it is comparable to that observed in other studies in low- and middle-income countries. For instance, a study done in the Philippines showed the rate of BCS was 11.6 % (15 out of 129 patients).13 In another study conducted in Soweto, South Africa, only 20% of patients were treated by BCS.15
Different blue dyes are used for SLNM, such as methylene blue dye (MBD), Patent Blue Vial (PBV) dye, and isosulfan blue. Our study used only methylene blue dye as it was the only blue dye available in our setup. The use of methylene blue is not without its risks, though; reports of allergic reactions, skin necrosis, and brief episodes of hypotension have been made in association with the use of this dye.13
The rate of identification of blue node (SLN) was 100% in our study. This is higher than results reported by other studies, such as one conducted in the Philippines, which showed a successful identification rate of 97.7%.13 However, using radioisotope and blue dye together (dual method) has a higher sensitivity as compared to using the blue dye method alone ( 95–100% vs 81–82%).16,17 In our study, the small study population could have contributed to the high identification rate of blue nodes. Using standard protocols, SLNs should be identified in > 95% of patients undergoing SLNB, with a 5–10% false negative rate.17 Nonetheless, using blue dye for SLNB is the most efficient and plausible option in resource-limited areas.18
In this study, the median number of harvested SLNs was 2.3. In over 99% of patients, removing up to 5 SLNs was adequate to identify metastatic nodes. Although results from the ACOSOG Z0011 trial have shown that ALND has no benefit to patients with 1 to 2 positive SLNs, in our setup, we did standard ALND for all our patients due to the unavailability of frozen section examination and the long waiting line for adjuvant chest wall and axillary radiation therapy.19
Among the total number of patients included in our study, pathologic evaluation revealed metastases in 6 patients (30%). Three of these patients (50%) had metastasis only to SLNs. The other three patients (50%) also had metastasis to other non-SLNs. There was no skip metastasis. This could be explained by the multiple sections that performed an in-depth evaluation of SLNs compared to the standard H and E exams routinely conducted for LNs identified by ALND. Though we cannot make a statistically significant conclusion, which would require collecting more data, our study demonstrated that 50% of ALN-positive status patients only had SLN-positive disease, which could have been missed with the conventional examination of the LNs identified by ALND.
Limitations
The number of patients we have included in our study is limited and lacks the statistical power to make any representative conclusions. Nonetheless, we have reported the preliminary outcomes to share our experience and encourage other facilities to reproduce this practice and conduct further research. The study will continue to include additional patients in our institution and other institutions that want to collaborate with us.
Conclusions
This study was able to describe the experience of SLNB in managing BRCa patients for the first time in Ethiopia. The use of blue dye alone in SLNB in our institution was successful and can be employed in other institutions with limited resources, even without a nuclear medicine facility. In our institution, we reported the outcome of our ongoing study, demonstrating the feasibility of the method and the outcomes we identified so far.
Our study showed that SLNB was successful in all the patients, with an acceptable number of SLNs identified. This suggests that multiple sectioning of SLNs is extremely valuable to determine axillary metastasis, directly impacting subsequent management in resource-limited setups. Though collecting additional data would be required to make a statically acceptable conclusion, the outcomes of this study clearly showed that even if SLNB could not eliminate the use of ALND due to reasons stated earlier, it did, however, identify 50% of patients with LN metastasis that may have been missed with the conventional examination.
Acknowledgements
In Honor of Dr. Sukamal Saha
Dr. Sukamal Saha, MD, FACS, FRCSC, was a distinguished Fellow of the American College of Surgeons and the Royal College of Physicians and Surgeons of Canada. He was affiliated with McLaren Flint Medical Center, Genesys Regional Medical Center, Hurley Regional Medical Center, and Myungsung Comprehensive Specialized Hospital. He served as the Chief of the Division of Surgical Oncology at McLaren Flint Regional Medical Center and an Associate Professor at Michigan State University.
Dr. Saha’s dedication to surgical oncology research was profound, with over 200 publications and more than 100 presentations at prestigious conferences. His commitment to patient care and mentorship was exemplary, having guided many young surgeons during his four years at Myungsung Comprehensive Specialized Hospital.
Known for his mantra, “treat every patient as if you would treat your mother, father, brother, or sister,” Dr. Saha’s passing in June 2024, after a brief illness, leaves a significant void. His influence on our lives and the field of surgical oncology is immeasurable, and we remain forever indebted to his kindness and expertise.