




Introduction
Trauma is one of the leading causes of fractures and dislocations of the extremities. Other non-traumatic causes include those that may be secondary to certain pathologic processes such as malignancies, and nutritional deficiencies amongst others. Anterior shoulder dislocation is the commonest of all types of shoulder dislocation accounting for about 90-95%1 of cases with most cases being successfully managed with closed reduction. The severity and complexity of shoulder fracture dislocation are sometimes dependent on the mechanism of injury, type of fracture, or degree of dislocation. These variables are pivotal to the sparing or compromise of neurovascular structures around the affected bone. Though rare, there have been reported cases of vascular compromise and brachial plexus injury after anterior shoulder dislocation estimated at about 1% and 7%, respectively.2 We present in our report an open anterior shoulder dislocation with an unusual clinical finding.
Case presentation
Patient
The patient is a 46-year-old man who sustained injury to the left shoulder with associated laceration in the left axilla. He was sitting behind the driver of a saloon car which ran into a ditch lost control and somersaulted into the bush, there was a case fatality involving the driver at the site of the accident. He also sustained a closed injury to the ipsilateral femur but no associated head or chest injury. Initial treatment was at the referral hospital where he was resuscitated and had suturing of the left axilla laceration before referral to our center.
On clinical examination, the left shoulder was swollen with a sutured laceration in the axilla measuring about 14cm (Fig 1a). Loss of rounded appearance (deltoid contour) and sharp prominence of the acromion (“squaring”). There was incongruence of the left glenohumeral joint with empty left glenoid fossa. He was able to flex and extend the elbow with no wrist drop and a good hand grip. Distal pulses were preserved. The left leg was swollen and deformed at the mid-thigh with intact distal neurovascular function.

Management with open reduction and K-wire fixation
Plain radiographs of the left shoulder showed an anterior dislocation of the left shoulder (Fig 1b) and of the left thigh showed a comminuted fracture of left femur. Immediate treatment was to reduce the shoulder dislocation closed under conscious sedation and to work up the patient for closed intramedullary nailing of the left femur. Immediately after closed reduction of the dislocated shoulder, however, patient was noticed to have absent radial pulses and this raised suspicion of a possible axillary artery compression.

The shoulder joint was then re-dislocated and strikingly, the pulses returned with good volume comparable to the contralateral side. Impression at this time was a possible tight suturing of the axillary laceration causing a reduction in the axillary space and hence compression on the axillary artery after reduction of the dislocation. Hence, the sutured laceration was released and an attempt was made again at reduction of the dislocation. Despite this, the distal pulses vanished after the second attempt, and the shoulder was re-dislocated with the pulses restored afterward. Consequently, the patient was worked up for operative exploration.
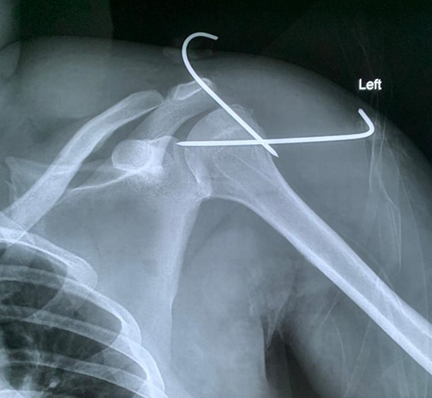
Intraoperatively, the left axilla was explored through the axillary laceration and intraoperative findings included an invaginated strip of skin (Fig 2a and 2b) behind the apposed and sutured wound at the referral hospital through which the humeral head buttonholed now compressing on the axillary artery once the shoulder was reduced. The strip of skin was excised (Fig 2c) and the dislocated shoulder joint was again reduced with preservation of the distal pulses. The glenohumeral joint was held reduced using K-wires (Fig 3) and the wound was copiously irrigated. A small, floating fragment of bone from the greater tuberosity not attached to any muscle was removed (Fig 1b and Fig 3) and closed using non-absorbable sutures. The patient subsequently had a closed intramedullary nailing of the left femur and post-operative course was uneventful.




Outcome and follow-up
Following surgery, patient was transferred to the lying ward for close monitoring. K-wire applied to the shoulder joint was removed four weeks post-operatively and patient was discharged to follow-up. Outpatient encounter since discharged has been uneventful.
Discussion
There have been reported cases of occlusion of the axillary artery following anterior shoulder dislocation though it is still a very rare phenomenon.3–7 The majority of the reported cases occurred however at the time of the anterior shoulder dislocation unlike in this case in which the occlusion occurred after reduction of the dislocation. A review of the literature and anatomy showed that the subscapular artery which is the largest branch of the distal part of the axillary artery and the posterior humeral circumflex artery are the two commonest branches of the axillary artery mostly implicated in axillary artery occlusion following anterior shoulder dislocation.3 This has been attributed to these arteries lying in the path of the dislocating humeral head. This was aptly demonstrated by Mckenzie and Sinclair by use of arteriogram in cadavers before and after dislocation.
In our case report however, intraoperative findings did not show occlusion of any of these branches of the axillary artery but rather compression of the axillary artery itself by a strip of invaginated skin through which the head of humerus buttonholed on reduction, this has not been reported in available English literature. This case also has a striking importance because the occlusion only occurred after reduction of the dislocation, and this has grave medico-legal importance. The importance of checking the distal pulses after reduction of a dislocation irrespective of the joint involved cannot be overemphasized as demonstrated in this case.
Ashton and Slaney8 reported two cases of iatrogenic axillary artery injury following reduction of a dislocated shoulder. In both cases, there was transection of the axillary artery which was subsequently repaired using an axillobrachial Teflon graft. One was as a result of an associated humeral neck fracture that was missed. This highlights the importance of requesting a plain radiograph for every suspected case of shoulder dislocation before attempting reduction and also a proper review of the radiograph so as not to miss any associated fracture.
One crucial lesson that could be drawn from this case is the importance of checking distal pulses before and after reduction of dislocation of large joints.
Conclusions
Anterior shoulder dislocation is common. Though rare, a strip of skin could cause vascular compromise after reduction thus, a proper clinical evaluation is mandatory, as well as immediate operative intervention. A high index of suspicion is therefore needed for early detection of any form of vascular compromise.